





Documentation Requirements

-
Description
No documentation = No coding = No billing

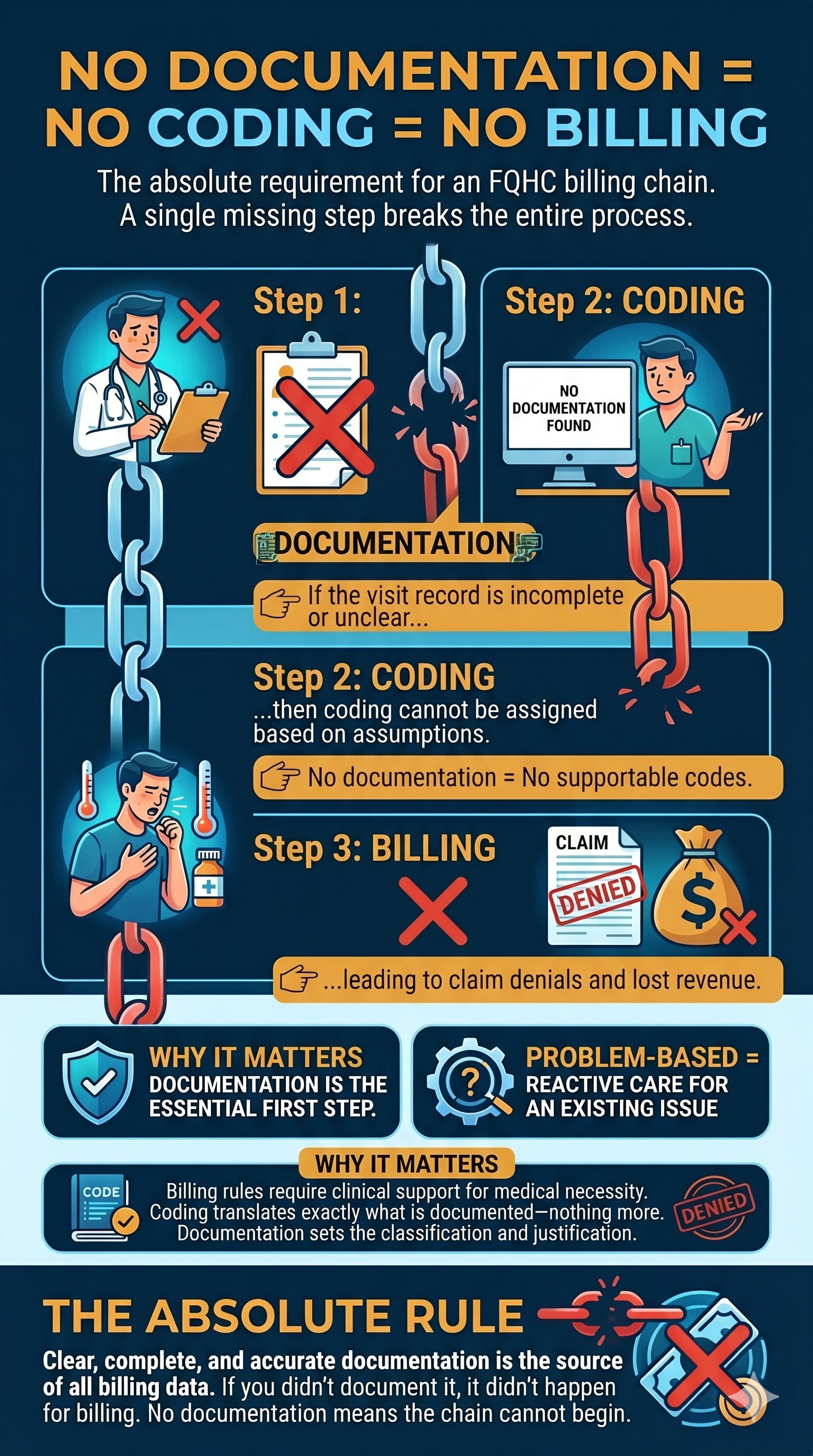
Why Complete Documentation Protects Every Claim
In medical billing, every patient visit must tell a complete and traceable clinical story. When even one key element is missing, the entire encounter becomes vulnerable to denial regardless of whether care was actually provided.
In the scenario, the visit was denied because the chief complaint was not documented, even though other parts of the record were complete. This highlights a critical reality in healthcare revenue cycle management: payers don’t bill based on intent or memory. They bill based on documentation.
Every visit must include:
- Chief Complaint – Why the patient came in
- Assessment & Diagnosis – Clinical findings and medical conclusion
- Treatment Plan – What was done or recommended
- Provider Signature – Proof of accountability and authentication
Core rule to remember:
No documentation = No coding = No billing
If it is not documented, it is treated as if it did not happen. Coders cannot assign codes without support, and billing teams cannot submit claims without validated documentation.
Key takeaway:
Complete documentation is not just compliance; it is the foundation of reimbursement. Every missing detail creates a gap in the story, and in medical billing, gaps lead to denials.